
Banal or not banal?
Since the beginning of the emergence of the coronavirus, I have been sharing my analysis that this is a rather ordinary epidemic. The term can be shocking when there are deaths, and even more so in the health crisis and the collective hallucinated drama we are experiencing. However, the facts speak for themselves : the common respiratory diseases that we experience every year cause somewhere around 2,600,000 deaths annually, worldwide. Now, four months into Covid-19, we are as of March 24 at less than 20,000 deaths, and the country initially the most affected (China) has managed to control the epidemic. The figures are far from showing a statistically significant effect with regard to the usual mortality and in particular to seasonal excess mortality.
I have said it before, and I will say it again: the same political or journalistic treatment applied to any episode of seasonal flu would terrify us just as much as the current epidemic. Just as the staging (with real-time counts of victims) of any major health problem, be it cardiovascular disease, cancer, or the effects of air pollution, would make us shudder with fright just as much, if not infinitely more!
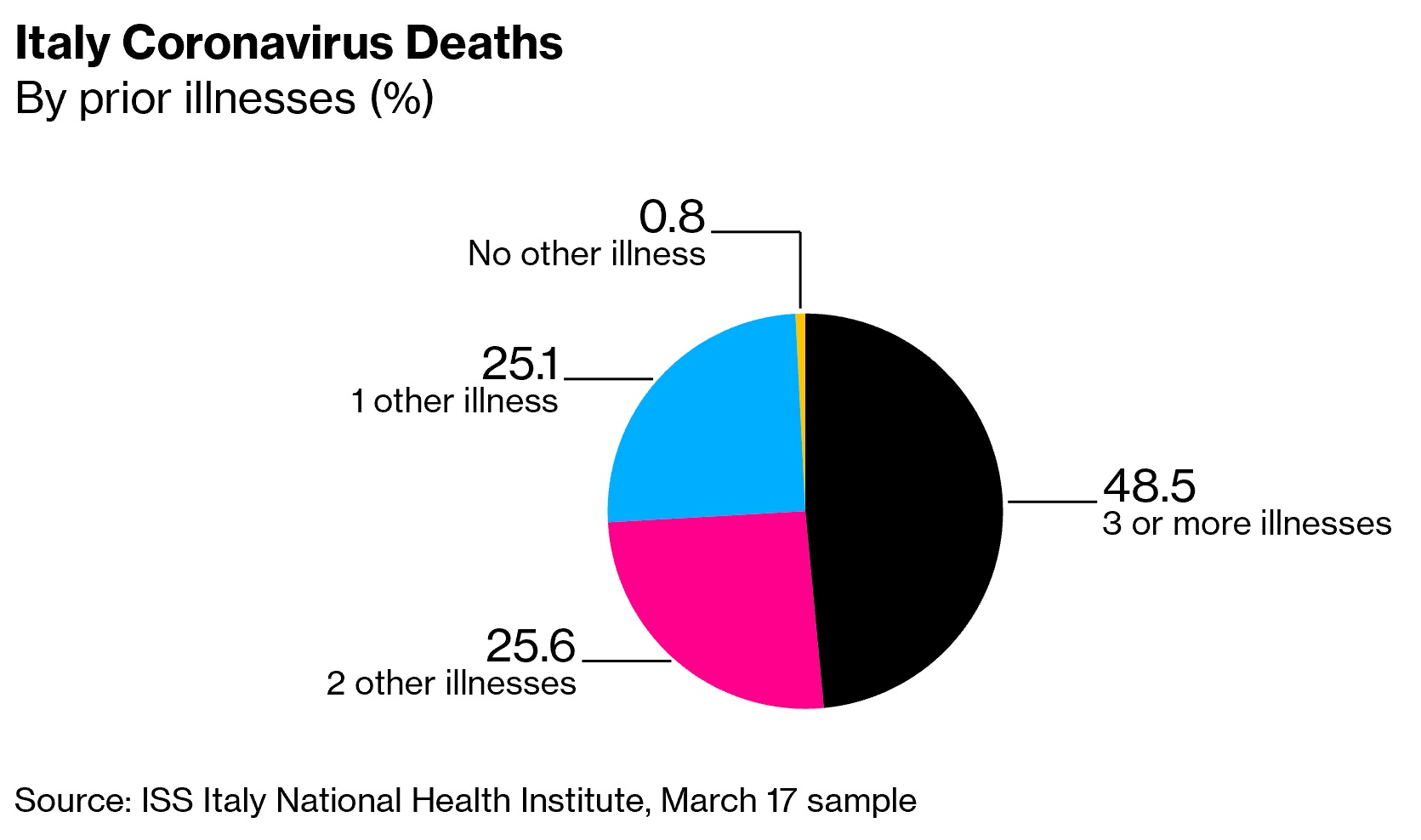
We now know that Covid-19 is benign in the absence of pre-existing pathology.
The most recent data from Italy confirm that 99% of the deceased suffered from one to three chronic pathologies (hypertension, diabetes, cardiovascular disease, cancer, etc.) with victims ageing 79.5 years on the average (median 80.5) and very few losses below the age of 65.
Stats and probs gone mad
There is another problem: the rates, especially those for complications and mortality, exhibited day in, day out, are meaningless. As long as there is no systematic testing of the population, we have no reliable data to which to refer the figures we obtain (the number of reported cases and of deaths).
This is a classic in epidemiology: if you only screen for deaths, you arrive at a death rate of 100%! If you only test the critical cases, the rate will be lower, but still much higher than the actual one. If you do a great deal of screening, you will find many cases, whereas if you do little testing, the number of cases will be low. The present cacophony just doesn’t give you any idea of how the virus is really progressing and spreading.
The most credible estimates suggest that the number of people who test positive for Covid is far lower than the number of people who are actually infected, about half of whom will not even realize they have contracted the virus. For a fearsome killer, it can be rather debonair at times…
At this point, then, we have no idea of the actual extent of the propagation of the virus. The good news is that the real figures (for percentages of complications and mortality) are necessarily much lower than the usual present claims. Actual mortality, as I announced in a previous paper, must be at 0.3% at most, and probably even lower. That is less than a tenth of the first figures announced by the WHO.
The latest models evaluate the minimum ratio between detected and undetected cases at 1:8 (and possibly at up to 1/47 or even lower depending on the screening strategies implemented in different countries. As of March 16, for example, the number of reported cases worldwide was established at 167,000, whereas the estimated overall number of infected individuals exceeded 1,000,000.
The detection rate is still low, even in countries that have massively adopted that strategy. While it remains impossible to know the number of unknown cases (!), this is still very far from the available statistics based on spotty data.
Is this the end of the world, or not ?
Similarly, most projections aimed at imagining the number of possible deaths are nothing short of madness. Many rest on an artificial, maximal “forcing” of all values and coefficients. They are established by people who work in offices, in front of computers, and do not have the slightest idea of the real world of field work or of clinical infectiology, resulting in absurd fictions. We might credit them with being creative and producing science fiction, but unfortunately their projections – literally psychotic – cause massive damage.
My experience in mental health makes me strictly avoid ready-made expressions such as “schizophrenia” or “psychosis”, which are almost always misused in a way that is derogatory to the people concerned. Medically speaking, psychosis is characterized by cognitive, perceptual and emotional distortions that lead to a loss of contact with reality. Here, unfortunately, the term is fully indicated.
I appeal to my colleagues in the Faculty of Medicine and other academic institutes to stop producing and peddling false, anxiety-provoking models. These experts protect themselves by recognizing, as a precaution of language, the excessive nature of their formalizations, while journalists scrupulously mention it (to their credit), but they are nevertheless just as diligently constructing the impression that the world is coming to an end. Not only is there absolutely no reason for this, but in addition, it is in itself profoundly harmful!
We can certainly give credit to our leaders for envisaging the worst of the worst of the worst on the basis of these fantasies so as not to take the slightest risk of it happening. In the meantime, we are constructing a (collective) hallucination on the basis of figures that mean nothing. The reality, once again, is that this epidemic is far less problematic and dangerous than what is claimed. It is the lack of an accurate policy that is hazardous.
OK, but what about all those deaths and those congested hospital departments?!
This is, alas, the real difficulty: were it not for those serious cases, the epidemic would be insignificant. It turns out that it leads to rare but dreadful complications. As Dr. Philippe Cottet, who is in the front line at the HUG (Geneva University Hospitals), wrote to me: “It must be said that viral pneumonia is usually extremely rare in Switzerland. The clinical picture is usually not clear-cut and the evolution sometimes fulminating, the warning signs of which are difficult to identify compared to more benign cases. It is a real clinical challenge, not to mention the number of simultaneous cases… »
It is the existence of these serious cases (absurdly estimated at 15% of cases, probably in reality 10 times less) that justifies not simply relying on herd immunity. The latter designates the process by which each person who contracts the virus and does not die from it becomes immune, while the multiplication of those immunized produces a collective effect of protective immunity…
In the absence – until recently – of any treatment capable of protecting or curing those at risk, the choice to let immunity build up by allowing the virus to circulate appeared to be too dangerous. The risk for vulnerable people is such that it would be ethically indefensible to move in this direction, given the seriousness of the possible consequences.
There is still the dramatic overcrowding in the emergency services due to the abundance of cases, and the major stress that it causes to health care teams left to their own devices and taking the full brunt of the reduction in resources over the last 20 years.
I understand the distress of the teams, as well as their possible anger at the elements that I am putting forward. Public health is profoundly different from clinical work, we do not work on the same scale. Each premature death is a tragedy suffered by health care teams, and I would sincerely be very sorry if I gave the impression of being indifferent to it. But we must do this work of contrast and granularity, looking at different scales to get to the bottom of the problem.
This is one of the difficulties of public health: both medicine and journalism work on particular cases. In medicine, that is why there is no “miracle cure”, for example. Each person may react differently to a treatment.
In journalism, the aim is to illustrate a topic with particular cases, thus showing images and words that are often shocking. In public health, we do not act at this singular “narrative” level. We collect data to see the exact contours of an issue. For example, on a global scale, the mortality rate for the under-60 age group is 1.8%. These cases do exist, but fortunately they are marginal.
One possible cause for concern, however, is the assertion that a significant number of young people are suffering from pneumonia and placed on respiratory assistance. Fortunately, they seem to survive, but it is the number of intensive care beds that is likely to be a problem if the overcrowding in the intensive care units continues.
A tragic paradox
It is in this complicated paradox between the great harmlessness of the virus for the vast majority of people and its extreme dangerousness in some cases that we found ourselves stuck. We then adopted measures that were absolutely contrary to good practice: we stopped screening people who might be ill, pleading for confining the population as a whole to stop the spread of the virus. These measures were actually medieval and problematic, since they only slowed down the epidemic at the risk of producing potentially even worse rebound phenomena. And too, they lock up everyone while only a small minority is affected. Conversely, all public health recommendations call for social distancing combined with detecting as many cases as possible, and confining positive cases only, until they are no longer contagious.
Confinement of everyone is a poor second-best way to deal with the epidemic, one that is due to the lack of everything that would enable us to fight it effectively…
Why did it come to this? Simply because we failed to set up the proper responses from the outset. The lack of tests and screening measures in particular is emblematic of this shipwreck: while Korea, Hong Kong, Taiwan, Singapore and China made these their top priority, we were unbelievably passive in organizing such technically simple action.
The above-mentioned countries have used artificial intelligence in particular to identify the possible chains of transmission for each positive case (smartphones, for example, can be used to inventory the movements and therefore the contacts that the infected people had with other people in the 48 hours preceding the development of symptoms).
Last, we have significantly reduced the capacity of our hospitals over the past decade and we are finding ourselves short of intensive care beds and resuscitation equipment. Statistics show that the countries most affected are those that have massively reduced the capacity of their intensive care units.
Percentage of beds for intensive care
Germany still has 6 beds for intensive care per one thousand inhabitants, as against 3.5 in Switzerland. This figure has dropped outstandingly in the Confederation over the last twenty years.
None of this has been the object of reflection, although the risk of a pandemic is a known major public health risk, in the face of which we are supposed to have prepared the right answers long ago. We found ourselves, although we should have been ready, lacking everything that would have been necessary to face the epidemic: not only screening tests, of course, but also basic sanitary material such as hydroalcoholic gels or protective masks for the nursing staff! The truth is that we have been completely overwhelmed.
One has only to look at the proven data for the countries mentioned to – hopefully – be able to admit that the losses are the consequence of our health plight. Singapore, in mid-February, was the second most affected country in the world after China, with the same number of “first-time” contaminants as later in Italy, France, Spain and Switzerland. One month later (22 March), only two deaths had been registered, all in all, compared to 5,476 in Italy!
The virus is obviously no different from one country to another! It is indeed the characteristics of the health policy response that make the difference between thousands of deaths and just a few. It is understandable that it is tempting or easier to play on war metaphors than to acknowledge our tragic unpreparedness…. The truth is that we have been completely overwhelmed.
Is the game over?!
The world’s leading expert on communicable diseases is Didier Raoult. He runs the Institut Hospitalier Universitaire (IHU) Méditerranée-Infection in Marseilles, which employs over 800 men and women. This institution possesses the most terrifying collection of “killer” bacteria and viruses in existence, and is one of the world’s leading centers of expertise in infectiology and microbiology. Professor Raoult is also ranked among the top ten French researchers by the journal Nature, both in terms of the number of his publications (over two thousand) and the number of citations by other researchers. Since the turn of the millennium, he has studied the various spectacular viral epidemics and has established close scientific contacts with the best of his Chinese colleagues. His achievements include the discovery of treatments (using chloroquine, in particular…) which are cited today in all handbooks on infectious diseases throughout the world.
On February 26th, he published a resounding video on an online channel (including the word “tube”) saying: “Coronavirus, game over! »
The reason for his enthusiasm? The publication of a Chinese clinical trial on the prescription of chloroquine, showing suppression of viral carriage in a few days on patients infected by SARS-CoV-2. Studies had already shown the efficacy of this molecule against the virus in the laboratory (in vitro). The Chinese study confirmed this efficacy on a group of affected patients (in vivo). Following this study, the prescription of chloroquine was incorporated into the treatment recommendations for the coronavirus in China and Korea, the two countries that have been most successful in controlling the epidemic…
Chloroquine has been on the market since 1949. The molecule is widely used as an antimalarial drug. All travelers to tropical countries will remember the Nivaquine tablets (one of its trade names) that were prescribed to them as a preventive measure against malaria. This remedy was later replaced by others for certain geographical areas, remaining in use for some destinations.
Hydroxychloroquine (trade name: Plaquenil) was prepared in 1955 and has a hydroxylation on one of the two ethyl groups in the side chain.
So what?!
Why am I talking about this? Well, because Professor Raoult and his co-workers are the best specialists in the world today in the use of chloroquine. In particular, he had the brilliant idea of testing its action against intracellular bacteria (which, like viruses, are capable of penetrating cells), in particular Ricksettia. The Marseilles IHU therefore has unparalleled clinical and pharmacological experience in the use of this molecule.
Chloroquine has also demonstrated its powerful therapeutic efficacy against most coronaviruses, including the dreaded SARS of sinister memory. The Chinese clinical trial therefore confirmed Raoul’s hypothesis that chloroquine could also be used against the Covid-19.
However, he was greeted as completely irrelevant; his colleagues denigrated his proposal from the outset. Le Monde, a daily newspaper, even went so far as to describe his communication as “fake news”, an accusation that was repeated on the Ministry of Health website for a few hours before being withdrawn.
Prof. Raoult was however immediately authorized to conduct a clinical trial on 24 patients in his department and was called to be part of the multidisciplinary committee of 11 experts set up in March by the French executive in order to “inform public decision-making in the management of the health situation related to the coronavirus.”
The results of the clinical trial were eagerly awaited, first and foremost by yours truly. We are well aware of how cautious one must be when faced with promising substances and how important it is to avoid any assertions before research has confirmed – or not – a hypothesis. Science is neither guesswork nor magic, it means observation, testing and then, if possible, validation.
The results of his clinical study came out on March 16, confirming that spectacular therapeutic effects have been obtained. The methodology is solid, since the Marseilles IHU was able to compare the negativation of viral carriage in patients who followed the protocol with patients in Avignon and Nice who did not receive that treatment.
“Those who did not receive Plaquenil [a hydroxychloroquine drug] were still carriers after six days in 90% of cases, while 25% of those who received treatment were positive,” explains Professor Raoult.
But it doesn’t stop there: the IHU Méditerrannée-Infection (like others) has long been advising that antibiotics be prescribed concomitantly for respiratory viral infections “because they are mainly complicated by lung disease. So all people who had clinical signs susceptible of evolving into a bacterial complication of pulmonary disease were given Azithromycin. There is proof that this lowers risk in people with viral infections. The other reason is that laboratory testing shows Azithromycin to be effective against a great many viruses, although it is an antibiotic. So if we were to choose an antibiotic, it was preferable to administer one that was effective against viruses. And when you look at the comparative percentage of positive carriers with the combination of hydroxychloroquine and Azithromycin, you find an absolutely dramatic decrease in the number of positive carriers “, he adds.
Viral carriage?
In the meanwhile, a study published in the Lancet on March 11 revealed a new but essential fact: the viral carriage period (time between the beginning and the end of the infection – and therefore possible contagiousness) is higher than previously thought, with an average duration of 20 days. With the hydroxychloroquine / azithromycin combination, this duration is reduced to 4-6 days.
The drastic reduction in viral carriage time not only gives us the hope that critical cases may be treated, but it also reduces the time it takes for an infected person to cease to be contagious. And this offers enormous prospects for preventing the spread of the virus. This news is of course the best news we could hope for. The authorities and scientists therefore welcomed it with joy, you would think…
Well, not by a long shot! The reactions that were first heard ranged from stupid to nasty.
Admittedly, neither the Chinese studies nor the clinical trial in Marseilles has the value of proof (“evidence”) according to the criteria of scientific research. Replication of the results by other teams is required, not to mention a randomized double-blind study, the top of the pop of research methodologies.
But what the hell! We are in an emergency situation. Chloroquine is one of the best known and best controlled drugs (in particular by the IHU in Marseilles). We can therefore be sure specialists possess very solid experience in prescribing it. Taking refuge behind procedural fundamentalism is ethically indefensible when we are talking about a drug that we know by heart, which has already demonstrated its efficacy on other coronaviruses, confirmed on this one by two clinical trial, and when lives are at stake day after day!
Raoult noted caustically that it was not impossible that the discovery of a new therapeutic utility for a drug that had fallen into the public domain long ago would be disappointing for all those hoping to win a Nobel Prize thanks to the breakthrough discovery of a new molecule or vaccine… Not to mention the prospect of tens of billions of dollars in revenue to be made, whereas chloroquine costs literally nothing.
In praise of caregivers!
For the past few days, the confined population has been speaking out every day to pay homage to caregivers and support them in the trying circumstances they are experiencing. This is a beautiful expression of solidarity, obviously well-deserved by these professionals, remarkable for their abnegation and commitment, in the face of this terrible suffering and new danger.
Unfortunately, the situation is far less admirable among our leading experts. Medical research and medical authority are also often made up of petty, manipulative, dishonest or abusive practices of all kinds, as well as pitiful but violent clashes of egos.
On a famous French news channel, BFM TV, Dr. Alain Durcadonnet immediately denigrated Raoult, reminding us that scientific findings should be published in scientific journals and not put on video… And he did this just when Prof. Raoult (who, I repeat, is the most frequently published researcher in scientific journals in his field) had of course just made it clear that a paper describing his clinical trials had been submitted to a peer-reviewed journal for publication. This anecdote like the following ones, shows how low some have dropped.
On March 1st, well after the publication of the first clinical trial in China, the Director General of Assistance Publique – Hôpitaux de Paris, Martin Hirsch, said on radio Europe 1 : “Chloroquine works very well in a test tube, but it has never worked in a living being”, which was already perfectly false!
In reports in the French national press, heavy emphasis is placed on the risk of overdosing with chloroquine, which is indeed toxic at doses exceeding 2 g/day in the absence of any concurrent somatic disorder. The Chinese preferred doses of 2x 500mg/day during their trial. Raoult and his team found this dosage excessive and preferred to opt for 600mg/day. The objection is therefore dismayingly unfounded – let us recall that no-one knows that molecule better than the Méditerranée-Infection clinical team. It would be like telling a team of neurologists working with Dafalgan: ooh there, be careful, it can be toxic if misused, so it’s really not a good idea to consider treating headaches with this drug!
There has been talk about its “toxicity” (yes indeed, read the press!), whereas hydroxychloroquine is a remedy for which we know all the risks. To which Raoult replied on March 21 with a post “Toxicity Chloroquine-Azithromycin a French nerve attack“, citing a 2011 study on the prescription of hydroxychloroquine to 755 pregnant women.
There was also talk about the risks associated with prolonged use, whereas the proposed treatment lasts an average of 7 days. Furthermore, the IHU has experience in administering exceptionally long-term prescriptions (up to two years!) for the treatment of some intracellular bacteria. We know that it is good to be charitable with our fellow man, but sometimes stupidity combined with dishonesty makes it difficult.
Others maintained (and still do) that no definitive conclusions can be drawn on the basis of clinical trials. This is quite right in the absolute, but does not apply to the present case, since this molecule is perfectly well known ! Raoult summarizes this absurd situation as follows : “There is a health emergency and we know how to cure the disease with a drug that we know perfectly well. We must be clear on where our priorities lie.” Given the reality of the epidemic, he recommends that we stop panicking and start detecting the ill without waiting for their case to get worse in order to give them a better treatment.
The problem goes beyond that…
Is this the loneliness of an extremely competent man? Raoult tells how Emmanuel Macron came looking for him after his first public announcement on February 26th, and his strange experience since then, within the circle of experts who advise the martial president. When asked by a journalist from Marianne: “Are you heard there? “, he replied: “I say what I think, but it is not translated into action. They call them scientific committees, but they are political. I’m like an alien there. »
It is his conviction, obviously uncomfortable for the authorities, that the measures currently applied to fight the epidemic are absolutely counter-productive. Romance-speaking European countries (unlike the Chinese and Koreans) have given up systematic screening, preferring a containment system that has never been an effective response to epidemics, as Professor Raoult stresses. This is an ancestral reflex of confinement (as in the times of cholera and in Giono’s book, “The Horseman on the Roof “). Confining people who are not carriers of the virus to their homes is infectiologically absurd – the only effect of such a measure is to destroy the economy and social life. A bit like bombing a city to keep malaria-carrying mosquitoes away…
The only procedure that makes sense, he says, is to confine carriers of the virus only, and to treat them if necessary either to avoid terrible complications like the ones presently seen or to reduce the time they are contagious.
In Switzerland as in France, Italy, Spain and many other countries in the West, the decision taken is to confine people to their homes as much as possible, sick or not. When they are sick, we wait for them to get better and then (because of the length of time they carry the virus), we let them out while they are still contagious! People at risk sometimes develop complications, especially acute respiratory distress, which leads them to the emergency room. They then clog up the intensive care units and some patients die there, whereas Raoult says they could have been treated before that!
Confining the entire population without screening and without treatment is on a par with the way epidemics were treated centuries ago.
The only strategy that makes sense is to screen massively, then confine the positive cases and/or treat them, as well as high-risk cases, since this is possible, as may be seen in China and Korea, whose treatment guidelines include a combination of massive screening and the prescription of chloroquine, included in their treatment guidelines.
Neither Hong Kong nor Taiwan nor Korea nor Singapore, territories with the lowest mortality rates for Covid-19, have imposed confinement on healthy people. They have simply set up a different organization.
Western decadence
Unfortunately, this decadence is glaring, and unequivocally revealed in this crisis… We have high quality medicine, but a medieval public health system. Technological and scientific leadership has gone over to the Far East long ago, and our intellectual self-centeredness often makes us cling to the lanterns of the past rather than to present-day science.
Systematic testing would be easy to implement, provided it is made a health priority and organized, which the Koreans have done in record time. In Europe, we are completely out of our depth, as if we were living in another age. The authorities now understand that this is an absolute priority – in line with the WHO’s insistent recommendations.
There is no difficulty in producing the tests: “It’s an ordinary PCR [polymerase chain reaction] that anyone can do, the problem is organization, not the technique or the diagnostic capability, we have that, says Raoult. It’s a choice, and that strategy is not chosen by most technologically advanced countries, whereas the Koreans, along with the Chinese, are among those who have controlled the epidemic through screening and treatment. In this country, and everywhere, we are capable of doing thousands of tests and testing everyone.”
Of course, more disciplined or even authoritarian political regimes have an advantage, with respect to social compliance, but that is not the point. The problem is definitely us. France has plunged into endless polemics before anyone has even opened their mouth, while its Jupiterian president indulges in flights of antiquated oratory about the “state of war” while contemplating himself in a mirror… In Switzerland, the Federal Council reacted calmly and benevolently, but gave the impression, as always, that it had been disagreeably awakened from its nap.
In short, for Switzerland, which prides itself on its innovations and high-quality biotech, we are still somewhat at a village party level.
Change is now?!
Luckily, we can expect a rapid, positive change of mind. The French Ministry of Health has just commissioned the Lille University Hospital to conduct a trial aimed at replicating the results obtained in Marseilles. Let’s remember that conclusive trials have already been conducted in China and Korea – but in France it is generally held that what comes from abroad is unworthy of French genius.
Interest in chloroquine is henceforth worldwide, and teams are working on it everywhere. If the drug proves its efficacy, as now seems most probable, this will be a major game-changer.
Once the individuals at risk for complications are diligently treated, the innumerable benign SARS-CoV-2 infections which so many of us will experience will provide the mass immunity which will reduce this “pandemic” to the size of a nasty misadventure.
Mass screening is at last a health priority now. Once we have provided laboratories with the capacity to do analyses, we will all be tested. Moreover, Sanofi pharmaceuticals has offered to produce one million doses of chloroquine free of charge to the French administration.
Finally, on 22 March, when the government had enjoined them to return to the ranks, Raoult and six of his colleagues imposed their legitimacy based on the Hippocratic Oath and the scandalous passivity of the public authorities:
In the current context of the spread of the Covid-19 coronavirus epidemic on French territory and throughout the world.
In accordance with the Hippocratic Oath we have taken, we are obeying our duty as doctors. We provide our patients with the best possible care for the diagnosis and treatment of a disease. We respect the rules of the art and the most recently acquired data of medical science.
We have decided:
– For all febrile patients who come to us, to perform the tests for the diagnosis of Covid 19 infection;
– For all infected patients, many of whom have only mild symptoms of lung damage on CT scans, to offer the earliest possible diagnosis of the disease:
– treatment with a combination of hydroxychloroquine (200 mg x 3 per day for 10 days) + Azithromycin (500 mg on the first day then 250 mg per day for 5 more days), as part of the precautions for use of this combination (with in particular an electrocardiogram on D0 and D2), and outside the MA. In cases of severe pneumonia, a broad-spectrum antibiotic is also associated.
We believe that it is unethical that this combination is not systematically included in therapeutic trials for the treatment of Covid-19 infection in France.
Pr Philippe Brouqui, Pr Jean-Christophe Lagier, Pr Matthieu Million, Pr Philippe Parola, Pr Didier Raoult, Dr Marie Hocquart
What if it doesn’t work?
But what if the molecule does not live up to expectations? This is of course a possibility, even if it is unlikely at this stage. Other drugs are currently under review, including those that are part of a major international, multi-center research effort to test antiviral molecules: remdesivir, lopinavir and ritonavir in combination, the latter administered with or without interferon beta. The research includes hydroxychloroquine, studied according to the protocol recommended by Raoult in several centers of expertise in clinical infectiology such as Oxford University and the University of Minnesota.
What is striking in the chloroquine issue is the religious fervor that pervades debate on this option – actually this is a classic in science. Raoult is depicted as a sort of guru (in spite of his remarkable scientific credentials), and there are descriptions of “belief” in the drug as the expectation of some “miracle drug” that misleads people, entertaining “impossible hopes”.
Fortunately, we have something called scientific method, which aims precisely at moving from the register of opinions (we each have our own views) to knowledge (what has been tested, checked, and verified independently of personal opinions).
If the results obtained in Marseilles and China are refuted, then the collective hallucination in which we have all been plunged will continue, with tremendously serious consequences for our society, our ways of life, our mental and social life. If, on the other hand, they are corroborated, we will have taken a giant step towards getting out of this awful mess, and then, the game will really be over for the Covid. And we will have learned a lot along the way.
A homage to the authorities
I am not accustomed to being accommodating with the authorities. Too often have I seen the ravages wrought by flattery and spinelessness (such as gratuitous criticism or attacks based on supposed motivations) to fall into that trap. Here in Switzerland we hear much criticism that seems unfair to me. No, we don’t really have a health system, so to speak, we have a sickness industry – that’s not the same thing. Yes, our sanitary responses are incredibly old-fashioned and in fact outdated. Yes, the Federal Council is lead-footed, and that has its advantages at times.
But I must say that I view the reaction of the Swiss federal and cantonal authorities as proportionate to what we know and what we do not know. It is easy to say we should have closed our borders a month ago, in a world in which the threat was as yet scarcely visible and in which we would have been the only ones to do so.
To close everything down unavoidably leads to economic and social disaster. Given the lack of means to apply the best strategy (detection – confinement – treatment), resorting to a lock-down is archaic and hardly effective, but it was the only one possible.
In Geneva in particular, the Conseil d’Etat (with Messieurs Mauro Poggia and Antonio Hodgers in the front line) was solid, human, reassuring, and clear, acting calmly with an undeniable sense of proportionality.
Once the emergency is over, however, the health and political officials will have to account for the fact that they turned out to be totally unprepared for a perfectly identified health risk, in a situation which is actually not very serious in comparison with the damage a really lethal pandemic would wreak.
Remember, the risk of a pandemic has been present and feared for over 30 years. It was to come from the Far East, but could, henceforth, come from the subarctic tundra where countless varieties of viruses previously frozen under the permafrost may now be freed.
It is somewhat as if no-one, in area threatened by earthquakes, had thought of promulgating anti-earthquake standards for buildings, or procedures to protect the population ! And all the while, hordes of senior officials and academics were generously paid to anticipate those risks.
We will also need to know why no-one was able to respond quickly and effectively (as some other countries did) to obtain, by requisitioning, if necessary, the industrial and scientific resources to do what had to be done. As one reader told me, France is, after all, the world’s top producer of respirators, and it has a powerful pharmaceutical industry.
One last piece of information, which should, I hope, encourage us to be cautious: the latest findings in infectiology seem to confirm the fact that children are very rarely carriers and/or contaminators of the SARS-CoV-2. If this hypothesis is corroborated, it would not be necessary to close schools, in fact. These findings date back to mid-march When the decision to close schools was made it was a precautionary measure, as I said in my previous blog, and the need for it might not exist if these findings are corroborated.
So, we must be patient and careful. Once this collective hallucination is over, it will be time to operate a very strict “post-mortem” examination of health-related decisions, and to try to understand what it took to generate such an incredibly wasteful societal mess.
The full version of this abridged article can be read HERE.